
Abstract
Haemoglobin C, which carries a glutamate-to-lysine mutation in the β-globin chain, protects West African children against Plasmodium falciparum malaria1,2. Mechanisms of protection are not established for the heterozygous (haemoglobin AC) or homozygous (haemoglobin CC) states. Here we report a marked effect of haemoglobin C on the cell-surface properties of P. falciparum-infected erythrocytes involved in pathogenesis. Relative to parasite-infected normal erythrocytes (haemoglobin AA), parasitized AC and CC erythrocytes show reduced adhesion to endothelial monolayers expressing CD36 and intercellular adhesion molecule-1 (ICAM-1). They also show impaired rosetting interactions with non-parasitized erythrocytes, and reduced agglutination in the presence of pooled sera from malaria-immune adults. Abnormal cell-surface display of the main variable cytoadherence ligand, PfEMP-1 (P. falciparum erythrocyte membrane protein-1), correlates with these findings. The abnormalities in PfEMP-1 display are associated with markers of erythrocyte senescence, and are greater in CC than in AC erythrocytes. Haemoglobin C might protect against malaria by reducing PfEMP-1-mediated adherence of parasitized erythrocytes, thereby mitigating the effects of their sequestration in the microvasculature.
Similar content being viewed by others


Main
Malaria continues to kill more than a million African children annually. Over thousands of years, evolutionary pressure has selected a variety of haemoglobin mutations that confer resistance to severe manifestations of the disease3. The mechanisms by which these mutations exert their influence are largely unclear. Haemoglobin C (HbC) contains a glutamate-to-lysine mutation at the sixth position in the β-globin chain, the same position as the glutamate-to-valine mutation in sickle haemoglobin (HbS). HbC occurs mostly in West Africa, where its prevalence in some regions is more than 25% and greatly exceeds that of HbS4. Epidemiological studies have shown substantial malaria protection by both the AC and CC phenotypes in the Dogon and Mossi ethnic populations of Mali and Burkina Faso1,2. Although reduced parasite proliferation in CC erythrocytes has been proposed as a mechanism of protection5,6, P. falciparum grows normally in AC erythrocytes in vitro5. Furthermore, the frequent presence of substantial parasite densities in malarious AC and CC children indicates that a process of protection other than reduced proliferation must operate in vivo1.
P. falciparum parasites remodel their host erythrocytes extensively, placing PfEMP-1 cytoadherence proteins in knob-like protrusions at the surface of the host cell membrane. These cell-surface modifications enable mature parasitized erythrocytes to sequester in the microvasculature and avoid clearance from the bloodstream by the spleen. The adherence properties of parasitized erythrocytes can lead to life-threatening manifestations of disease—accumulation of parasitized erythrocytes in the brain, for example, produces the clinical syndrome of cerebral malaria7. Because of this link between erythrocyte-surface modifications and disease, we compared P. falciparum-infected AC, CC and AA erythrocytes in assays of cytoadherence, rosetting and agglutination, three phenomena that depend on PfEMP-1 expression at the host erythrocyte surface8,9.
In the first of these comparisons, we tested the ability of parasitized erythrocytes to adhere to endothelial monolayers expressing two important host cytoadherence receptors, CD36 and ICAM-1. Under flow conditions10, parasitized AC erythrocytes showed ∼25% reduced adherence to these endothelial monolayers compared with parasitized AA erythrocytes, and parasitized CC erythrocytes showed no adherence (Fig. 1a).

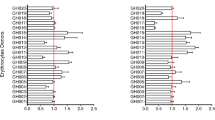
a, Adherence of parasitized AA, AC, and CC erythrocytes to human dermal microvascular endothelial cell (HDMEC) monolayers under flow conditions. b, Rosette frequencies of erythrocyte samples (4 AA, 3 AC, 1 CC) parasitized with P. falciparum lines (MC/R+ or TM284). c, Agglutination scores from erythrocyte samples (5 AA, 2 AC, 3 CC) parasitized with P. falciparum lines (7G8, GB4, FCR3 or MC/R+) and tested with eight antisera (not all combinations used). d, Agglutination scores of erythrocyte samples (5 AA, 2 AC, 3 CC) parasitized with P. falciparum lines (7G8 or GB4) and tested with three antisera at serial dilutions. e, Agglutination scores of naturally infected AA and AC erythrocytes from Malian children. Error bars show s.d.
Rosette formation by attachment of non-parasitized to parasitized erythrocytes is likewise mediated by PfEMP-1 and involves host cell receptors, including complement receptor 1 (ref. 9). Increased rosette frequencies are associated with increased malaria severity11. Using two different P. falciparum lines, we found that rosette frequencies were ∼33% lower for AC erythrocytes compared with AA erythrocytes, and that rosettes formed only rarely with CC erythrocytes (Fig. 1b).
In our third set of comparisons, we tested unfixed parasitized erythrocytes for their ability to agglutinate in the presence of serum from individuals with immunity to malaria. This clumping in response to antibody–antigen interactions is a sensitive assay for the cell-surface expression of PfEMP-1 (refs 8, 12, 13). Immune sera agglutinated parasitized AC erythrocytes significantly less than parasitized AA erythrocytes, and agglutinates of parasitized CC erythrocytes were infrequent (Fig. 1c). Marked relative reductions occurred over a wide range of serum dilutions, confirming that the results had not been compromised by non-optimal ratios of antibodies to parasite antigens (Fig. 1d). These data are consistent with reduced antibody bridging of PfEMP-1 molecules between parasitized HbC erythrocytes.
To test whether HbC affects PfEMP-1-mediated phenomena in vivo, we studied parasitized AC and AA erythrocytes obtained directly from Malian children with malaria. After placing these samples in culture for 24 h to allow for the development of late-stage parasites expressing PfEMP-1, we tested for agglutination using sera pooled from nine immune adults in the same village. The parasitized erythrocytes from 19 out of 20 AA children agglutinated, confirming broad reactivity of the adult serum pool (Fig. 1e). In contrast, three out of three infected AC samples did not show sufficient numbers of agglutinates to yield a positive agglutination score. The mean agglutination scores of parasitized AC and AA erythrocytes were significantly different (0.0 versus 1.6; P = 0.005). In parallel experiments, we purified P. falciparum trophozoites from AA samples that had yielded agglutination scores of 4 and then inoculated the recovered parasites into fresh AC erythrocytes (two donors) or CC erythrocytes (three donors). After a single two-day cycle of reinvasion and growth, the resulting trophozoite-infected AC or CC erythrocytes gave agglutination scores of zero, providing additional evidence for an important effect of HbC on the antibody–PfEMP-1 bridges between parasitized erythrocytes. This effect appeared to involve PfEMP-1 display specifically, as control experiments showed no differences between the agglutination of AA, AC, and CC erythrocytes using standard ABO/Rh blood typing antibodies.
Altered adherence properties of HbC erythrocytes relative to AA erythrocytes could be due to reduced levels of PfEMP-1 or to its altered distribution in knobs, both of which can exert important influences on the organization and cooperativity of PfEMP-1 interactions with attaching molecules14. To explore these possibilities, we used flow cytometry to examine unfixed parasitized erythrocytes for their reactivity to rat antisera against different forms of PfEMP-1 expressed by the mature trophozoite stages of two P. falciparum lines, MC/R + and FVO. Forty-eight hours after infection with purified, synchronized trophozoites, populations of AA and AC erythrocytes showed overlapping distributions of fluorescence, with parasitized AC erythrocytes showing ∼15% lower median fluorescence intensities (MFI) (Fig. 2 and Supplementary Table 1; mean AC:AA MFI ratio ± s.d. = 0.85 ± 0.10; P < 0.0001, two-tailed, one sample t-test of the mean). MFIs from parasitized CC erythrocytes were markedly lower (Fig. 2c, f and Supplementary Table 1; mean CC:AA MFI ratio ± s.d. = 0.33 ± 0.12; P < 0.0001). Notably, the MC/R + and FVO P. falciparum lines consistently showed significant differences in their expression of PfEMP-1 on CC erythrocytes (Fig. 2c, f; 8% of parasitized erythrocytes expressing PfEMP-1 for MC/R + compared with 38% for FVO). These findings might reflect differing abilities of P. falciparum lines to develop in and remodel the surface of CC erythrocytes in vitro6, and raise the possibility that protection against malaria by HbC is strain-dependent.

a–f, Parasitized erythrocytes were stained with ethidium bromide (EtBr) and probed with a rat polyclonal antiserum specific for an extracellular PfEMP-1 molecule of P. falciparum line MC/R + (a–c) or FVO (d–f). Parasitized erythrocytes reactive to antisera appear as clustered populations in the upper right quadrants (red numbers indicate MFI). Upper left quadrants include signals from parasite populations that express variant PfEMP-1 molecules not reactive with antisera. Percentage figures in the upper quadrants were calculated from the total erythrocyte number in each sample.
In parallel with flow cytometry, we used confocal microscopy to examine the distribution of PfEMP-1 on the surface of fresh AA, AC and CC erythrocytes infected with comparably mature P. falciparum trophozoites. Deconvoluted confocal images and cell-surface stack projections showed uniform and finely distributed signals from PfEMP-1 over the surfaces of AA erythrocytes (Fig. 3a). Parasitized CC erythrocytes yielded fluorescence intensities that were often weaker and showed irregular and widely dispersed PfEMP-1 distributions (Fig. 3b). On AC erythrocytes, PfEMP-1 showed a spectrum of intensities and distributions that in some cases were AA-like (Fig. 3c) and in other cases were CC-like (Fig. 3d). The presence of significant numbers of parasitized AC erythrocytes with CC-like PfEMP-1 display (∼ 25% of the parasitized cells in our samples) is the probable explanation for the reduced MFI levels of AC populations measured by flow cytometry.

a–d, Confocal cross-sections through the midplane (left column) or maximum intensity projections of z stacks through the upper cell surface (right column) of trophozoite-infected erythrocytes probed with a polyclonal antiserum against PfEMP-1 (FVO line). a, PfEMP-1 fluorescence patterns typical of a parasitized AA erythrocyte. b, Irregular, patchy PfEMP-1 distributions typical of a parasitized CC erythrocyte. c, Fluorescence patterns from a parasitized AC erythrocyte, similar to those of parasitized AA erythrocytes. d, Dispersed and brightly punctate fluorescence signals from abnormally displayed PfEMP-1 on an AC erythrocyte. e, f, Transmission electron micrographs of parasitized AC erythrocytes in continuous culture. Arrows indicate knobs that have a normal (AA-like) appearance (e) or abnormal (CC-like6) appearance (f). Some parasitized AC erythrocytes were also observed to have both normal and abnormal knobs (data not shown). g, h, Knobs with normal (g) or abnormal (h) appearance on a parasitized AC erythrocytes from a child with malaria. i–k, Scanning electron micrographs showing a normal uninfected AA erythrocyte (i), frequent knobs on a trophozoite-infected AA erythrocyte (j), and abnormally large and widely separated knobs on a similarly parasitized AC erythrocyte (k).
PfEMP-1 molecules are anchored in knobs placed by P. falciparum under the host erythrocyte membrane15, and their display at the cell surface is affected when knob placement and organization is abnormal14. We therefore evaluated the ultrastructural appearance of knobs on trophozoite-infected AA and AC erythrocytes using both transmission and scanning electron microscopy. In transmission electron micrographs, we observed distinct populations of parasitized AC erythrocytes: (1) a population with regularly distributed arrays of fine knobs resembling those of parasitized AA erythrocytes (Fig. 3e) and (2) a population with abnormally large, widely separated knobs that resembled those of parasitized CC erythrocytes6 (∼ 25% of the infected AC cells; Fig. 3f) and were not observed in control parasitized AA erythrocytes. We also examined parasitized erythrocytes drawn from malaria patients and cultivated within 30 h to mature trophozoite stages (Fig. 3g, h). These again showed that ∼25% of parasitized AC but not AA erythrocytes carried large and widely separated knobs (Fig. 3h). Scanning electron microscopy confirmed extensive remodelling of the surface of parasitized AA and AC erythrocytes relative to the smooth, biconcave surface of uninfected erythrocytes (Fig. 3i). The knobs on parasitized AA erythrocytes were numerous and finely distributed (Fig. 3j), whereas parasitized AC erythrocytes frequently had larger and widely separated knobs (Fig. 3k). Concordant appearance of these images with the patterns of immunofluorescence signals (Fig. 3a, d) is consistent with widely dispersed anchoring and irregular concentrations of PfEMP-1 in the knobs of parasitized AC and CC erythrocytes. Direct studies of PfEMP-1 distributions in relation to the knob topography of parasitized AC and CC erythrocytes, including examination by atomic force microscopy16, will be required to confirm and extend these observations.
The frequent presence of abnormal knobs on AC erythrocytes might be associated with the cellular changes of erythrocyte ageing17. Such age-associated effects include increases in cell density and mean corpuscular haemoglobin concentration (MCHC). AC erythrocyte populations contain 30–40% HbC and have MCHCs (34.2 ± 1.7 g dl-1) midway between the concentration in normal AA erythrocytes (31.8 ± 1.2 g dl-1) and the more dense CC erythrocytes (36.4 ± 1.4 g dl-1) (refs 18–20). The range of densities about these mean values allows separation of erythrocyte populations into high- and low-density fractions by ultracentrifugation in autologous plasma21. When we performed these separations and used transmission electron microscopy to examine the knobs of AC erythrocytes of different densities infected with mature trophozoites, we found that the proportion of parasitized erythrocytes displaying abnormal knobs was an average of 4 times greater in high-density than in low-density AC fractions (Fig. 4a; mean ± s.d. 40.5 ± 9.0% for high-density versus 10.5 ± 2.9% for low-density AC erythrocytes; P = 0.02).

a, Prevalence of abnormal knobs in low- and high-density erythrocytes from four different AC samples parasitized with P. falciparum clone 7G8. UfE, unfractionated erythrocytes; LDE, low-density erythrocytes; HDE, high-density erythrocytes. b, Hemichrome levels in low- or high-density fractions of erythrocytes from 3 AA, 3 AC and 3 CC donors. Error bars indicate s.d. c, Senescent antibody signals from freshly drawn erythrocytes of one AA, 4 AC and 3 CC donors. Three additional AA samples also gave no signal (data not shown).
Erythrocyte senescence is associated with the oxidation of haemoglobin to hemichromes, which lodge beneath the membrane of the cell and decrease its plasticity. Clustering of band 3 by hemichromes induces binding of autologous immunoglobulin, fixation of complement and opsonization of senescent erythrocytes22. We examined fresh AC and CC erythrocytes for elevated levels of hemichromes and membrane-bound autoantibody. Results showed increased levels of hemichromes in CC and high-density AC erythrocytes relative to AA and low-density AC erythrocytes (Fig. 4b). Surface autoantibody was detected on the erythrocytes of all AC donors and, at much higher levels, on those of CC donors; in contrast, AA erythrocytes carried no detectable autoantibody (Fig. 4c). An increased susceptibility of HbC to oxidation23 might underlie these and other cellular changes that compromise the ability of P. falciparum to remodel HbC erythrocytes.
PfEMP-1 has a central role in the cytoadherence and rosetting of parasitized erythrocytes and the effects of these phenomena in severe malaria24,25. We suggest that haemoglobin C affects the display of PfEMP-1 by reducing both its expression level and distribution at the host cell surface. These effects would in turn mitigate obstruction and inflammation resulting from the adherence of parasitized erythrocytes in the microvasculature, and might be complemented by an increased rigidity of HbC erythrocytes. This model of malaria protection by HbC has features independent of acquired immunity, and could therefore be implicated in the protection of young children and pregnant women, who often lack the variant-specific PfEMP-1 antibodies associated with clinical protection12,13,26. Varying spectra of PfEMP-1 abnormalities on parasitized AC and CC erythrocytes can help to explain why some children with HbC still suffer severe malaria and why the CC phenotype might afford greater protection than the AC phenotype, as some results have suggested2. As with other malaria-protective polymorphisms, such as those of sickle trait and glucose-6-phosphate dehydrogenase (G6PD) deficiency27, HbC protection can vary among human populations1. Effects of genetic background, parasite strain variations, regional patterns of disease transmission and incidence, nutritional status and acquired immunity all might influence the susceptibility of HbC carriers to severe malaria. Identification of factors that modify the AC and CC phenotypes will improve our understanding of malaria-protective mechanisms and help to explain their variable fitnesses across the mutant haemoglobin clines of Africa and southeast Asia4.
Methods
Red blood cells
Heparinized blood was washed with RPMI 1640 (Invitrogen/Gibco) and stored at 50% hematocrit at 4 °C before use. Haemoglobin genotypes were determined by cellulose acetate and citrate agar electrophoresis, and confirmed by high-performance liquid chromatography. Blood collection was approved by the Institutional Review Boards of the National Institute of Allergy and Infectious Diseases and the University of Bamako.
Parasite culture
Parasites in AA and AC erythrocytes were cultivated at 5% hematocrit in complete medium (RPMI 1640 supplemented with 25 mg ml-1 HEPES, 2 mg ml-1 sodium bicarbonate, 50 µg ml-1 gentamicin and 10% (v/v) heat-inactivated human O+ or AB+ serum). Parasites in CC erythrocytes were cultivated similarly but at lower (0.5–1.0%) hematocrit. This modification allowed us to maintain parasite cultures in CC erythrocytes that were synchronous with control cultures in AA erythrocytes (see Supplementary Table 2) and contained >90% viable forms, as determined by transmission electron microscopy. All cultures were maintained at 37 °C in an atmosphere of 5% CO2, 5% O2 and 90% N2, with twice daily medium changes. Erythrocytes were obtained in both the United States and Mali. In all experiments, age-matched AA, AC and CC erythrocytes were simultaneously inoculated by the same parasite stock within 4–48 h of blood collection, as described6. Parasites expressing knobs were maintained by periodic gelatin flotation6. P. falciparum-infected erythrocytes from Malian children were placed in culture for 24 h to allow development of late-trophozoite stage parasites suitable for agglutination assays (see below).
Flow cytoadherence assays
Human dermal microvascular endothelial cells (HDMEC) were harvested from discarded neonatal human foreskin samples following a protocol approved by The Conjoint Ethics Review Board of the University of Calgary. HDMEC were maintained in endothelial basal medium and grown to confluent monolayers as described10. Suspensions of parasitized erythrocytes (1% hematocrit, 5% parasitemia in RPMI 1640, pH 7.2) were drawn through a parallel-plate flow chamber at a rate producing shear stresses approximating those in the microvasculature10. After 7 min video recording, five additional fields were recorded (30 s each). Parasitized erythrocytes were considered adherent only if they remained stationary for more than 10 s. Mean counts were obtained from at least five microscopic fields and were expressed as the number of adherent parasitized erythrocytes per mm2 surface area. The numbers of infected AC and CC erythrocytes bound were calculated as percentages of the number of control infected AA erythrocytes bound. Experimental and control erythrocytes were tested simultaneously. Erythrocytes from two AA and two AC donors were infected with the P. falciparum 7G8 line and tested for binding on the same cell passage of two different HDMEC monolayer preparations. 7G8-parasitized CC erythrocytes were tested on three sequential passages of the same HDMEC preparation.
Rosetting
MC/R+ and TM284 parasites were cultured to 5–10% parasitemia in AA, AC and CC erythrocytes, as above. Erythrocytes containing mature parasites were identified by their refractile hemazoin pigment. Rosettes were identified as parasitized erythrocytes to which three or more uninfected erythrocytes were closely adhered. Absolute rosette rates were determined by dividing the total number of rosettes by the number of parasitized erythrocytes examined (> 200). Rosette frequencies (%) were calculated relative to the rosette rates of control parasitized AA erythrocytes.
Parasitized erythrocyte agglutination assays
Agglutination of parasitized erythrocytes (5% at mature-stage parasitemia) was tested and scored as previously described28. Immune sera included pooled adult serum samples from various regions of Africa endemic for P. falciparum malaria, and convalescent serum from Pan troglodytes experimentally infected with a genetic cross of the P. falciparum lines GB4 and 7G8 (unpublished). Use of relevant non- and pre-immune sera resulted in no agglutination.
Flow cytometry
Rat polyclonal antisera were raised against externalized segments of PfEMP-1 expressed by the MC/R+ and FVO parasite lines. Approximately 1 × 106 erythrocytes at 1% parasitemia were stained with antisera (anti-MC/R + at 1:80 dilution; anti-FVO at 1:800) in PBS containing 2% fetal calf serum for 30 min at 25 °C and washed. Bound antibody was detected using Alexa 488-conjugated anti-rat IgG (Molecular Probes). Parasitized erythrocytes were stained with ethidium bromide (2 µg ml-1) for 30 min. A FACSort instrument (Becton-Dickinson) and FlowJo software were used to acquire and analyse 500,000 events from each sample.
Surface immunofluorescence/confocal microscopy
Parasitized erythrocytes (2 µl packed cell volume) were added to 20 µl polyclonal antiserum (rat, 1:100 dilution, MC/R + ; 1:1,500 dilution, FVO) for 1 h at 25 °C and washed. Bound antibody was detected with Alexa 488-conjugated anti-rat IgG. Control experiments using antiserum against the intracellular acidic terminal segment (ATS) of PfEMP-1 gave no signal, confirming that the unfixed, parasitized erythrocytes in these experiments were not antibody permeable. Images were collected using a TCS-SP2 AOBS confocal microscope (Leica Microsystems) using a ×63 oil immersion objective NA 1.4, zoom 6. The confocal pinhole was set to 0.9 Airy units to ensure maximum resolution. Alexa 488 fluorescence was excited using an argon laser at 488 nm. DIC (differential interference contrast) images were collected using the same 488-nm excitation wavelength but with the transmitted light detector. 3-dimensional reconstructions were made using sequential sections through the sample with a z increment of 0.12 µm. Images were deconvoluted and processed using Leica TCS (version 2.1374), Imaris 4.1 (3-D reconstructions) (Bitplane AG), Huygens Essentials (deconvolution) (SVI) and Adobe Photoshop CS (Adobe Systems).
Electron microscopy
Parasites were processed for transmission electron microscopy as described6. The knobs of 50–200 trophozoite-infected erythrocytes were scored from each sample. For scanning electron microscopy, P. falciparum-infected AA and AC erythrocytes were washed in phosphate-buffered saline (pH 7.4), fixed in 2.5% glutaraldehyde plus 4% paraformaldehyde in 0.1 M sodium cacodylate/0.05 M sucrose. Samples were photographed at 5 kV using a Hitachi S-4500 field emission scanning electron microscope.
Density fractionation of AA and AC erythrocytes
Erythrocyte suspensions were adjusted to 90% hematocrit in autologous plasma and ultracentrifuged at 51,000g for 2 h at 25 °C (ref. 21). The top and bottom 10% or 25% volumes of packed erythrocytes were removed and used in parasite cultures or hemichrome extractions.
Quantification of hemichromes and detection of senescent antibody
Heparinized blood was washed in HEPES buffer, pH 7.4 (10 mM HEPES, 140 mM NaCl, 10 mM glucose) and the erythrocytes were lysed with Tris-HCl/EDTA (pH 8.0) in the presence of protease inhibitors (Complete; Roche Diagnostics GmbH). Membrane pellets were extracted as described29. Hemichromes were quantified using the Winterbourne equation30. For detection of senescent antibody, protein extract (1 µg) was resolved by SDS–PAGE, transferred to a PVDF membrane, and probed with a horseradish peroxidase-conjugated anti-human IgG antibody and chemiluminescent substrate.
References
Agarwal, A. et al. Hemoglobin C associated with protection from severe malaria in the Dogon of Mali, a West African population with a low prevalence of hemoglobin S. Blood 96, 2358–2363 (2000)
Modiano, D. et al. Haemoglobin C protects against clinical Plasmodium falciparum malaria. Nature 414, 305–308 (2001)
Flint, J., Harding, R. M., Boyce, A. J. & Clegg, J. B. The population genetics of the haemoglobinopathies. Baillieres Clin. Haematol. 11, 1–51 (1998)
Allison, A. C. Genetic factors in resistance to malaria. Ann. NY Acad. Sci. 91, 710–729 (1961)
Friedman, M. J., Roth, E. F., Nagel, R. L. & Trager, W. The role of hemoglobins C, S, and Nbalt in the inhibition of malaria parasite development in vitro. Am. J. Trop. Med. Hyg. 28, 777–780 (1979)
Fairhurst, R. M., Fujioka, H., Hayton, K., Collins, K. F. & Wellems, T. E. Aberrant development of Plasmodium falciparum in hemoglobin CC red cells: implications for the malaria protective effect of the homozygous state. Blood 101, 3309–3315 (2003)
Miller, L. H., Baruch, D. I., Marsh, K. & Doumbo, O. K. The pathogenic basis of malaria. Nature 415, 673–679 (2002)
Baruch, D. I. et al. Cloning the P. falciparum gene encoding PfEMP1, a malarial variant antigen and adherence receptor on the surface of parasitized human erythrocytes. Cell 82, 77–87 (1995)
Rowe, J. A., Moulds, J. M., Newbold, C. I. & Miller, L. H. P. falciparum rosetting mediated by a parasite-variant erythrocyte membrane protein and complement-receptor 1. Nature 388, 292–295 (1997)
Yipp, B. G. et al. Synergism of multiple adhesion molecules in mediating cytoadherence of Plasmodium falciparum-infected erythrocytes to microvascular endothelial cells under flow. Blood 96, 2292–2298 (2000)
Rowe, A., Obeiro, J., Newbold, C. I. & Marsh, K. Plasmodium falciparum rosetting is associated with malaria severity in Kenya. Infect. Immun. 63, 2323–2326 (1995)
Marsh, K., Otoo, L., Hayes, R. J., Carson, D. C. & Greenwood, B. M. Antibodies to blood stage antigens of Plasmodium falciparum in rural Gambians and their relation to protection against infection. Trans. R. Soc. Trop. Med. Hyg. 83, 293–303 (1989)
Bull, P. C. et al. Parasite antigens on the infected red cell surface are targets for naturally acquired immunity to malaria. Nature Med. 4, 358–360 (1998)
Crabb, B. S. et al. Targeted gene disruption shows that knobs enable malaria-infected red cells to cytoadhere under physiological shear stress. Cell 89, 287–296 (1997)
Oh, S. S. et al. Plasmodium falciparum erythrocyte membrane protein 1 is anchored to the actin-spectrin junction and knob-associated histidine-rich protein in the erythrocyte skeleton. Mol. Biochem. Parasitol. 108, 237–247 (2000)
Arie, T., Fairhurst, R. M., Brittain, N. J., Wellems, T. E. & Dvorak, J. A. Hemoglobin C modulates the surface topology of Plasmodium falciparum-infected erythrocytes. J. Struct. Biol. 150, 163–169 (2005)
Williams, A. R. & Morris, D. R. The internal viscosity of the human erythrocyte may determine its lifespan in vivo. Scand. J. Haematol. 24, 57–62 (1980)
Huisman, T. H. Chromatographic separation of hemoglobins A 2 and C. The quantities of hemoglobin A 2 in patients with AC trait, CC disease, and C-β-thalassemia. Clin. Chim. Acta 40, 159–163 (1972)
Bunn, H. F. et al. Molecular and cellular pathogenesis of hemoglobin SC disease. Proc. Natl Acad. Sci. USA 79, 7527–7531 (1982)
Charache, S., Conley, C. L., Waugh, D. F., Ugoretz, R. J. & Spurrell, J. R. Pathogenesis of hemolytic anemia in homozygous hemoglobin C disease. J. Clin. Invest. 46, 1795–1811 (1967)
Murphy, J. R. Influence of temperature and method of centrifugation on the separation of erythrocytes. J. Lab. Clin. Med. 82, 334–341 (1973)
Low, P. S., Waugh, S. M., Zinke, K. & Drenckhahn, D. The role of hemoglobin denaturation and band 3 clustering in red blood cell aging. Science 227, 531–533 (1985)
MacDonald, V. W. & Charache, S. Drug-induced oxidation and precipitation of hemoglobins A, S and C. Biochim. Biophys. Acta 701, 39–44 (1982)
Kaul, D. K., Roth, E. F. Jr, Nagel, R. L., Howard, R. J. & Handunnetti, S. M. Rosetting of Plasmodium falciparum-infected red blood cells with uninfected red blood cells enhances microvascular obstruction under flow conditions. Blood 78, 812–819 (1991)
MacPherson, G. G., Warrell, M. J., White, N. J., Looareesuwan, S. & Warrell, D. A. Human cerebral malaria. A quantitative ultrastructural analysis of parasitized erythrocyte sequestration. Am. J. Pathol. 119, 385–401 (1985)
Ricke, C. H. et al. Plasma antibodies from malaria-exposed pregnant women recognize variant surface antigens on Plasmodium falciparum-infected erythrocytes in a parity-dependent manner and block parasite adhesion to chondroitin sulfate A. J. Immunol. 165, 3309–3316 (2000)
Ruwende, C. et al. Natural selection of hemi- and heterozygotes for G6PD deficiency in Africa by resistance to severe malaria. Nature 376, 246–249 (1995)
Gamain, B. et al. The surface variant antigens of Plasmodium falciparum contain cross-reactive epitopes. Proc. Natl Acad. Sci. USA 98, 2664–2669 (2001)
Giribaldi, G., Ulliers, D., Mannu, F., Arese, P. & Turrini, F. Growth of Plasmodium falciparum induces stage-dependent haemichrome formation, oxidative aggregation of band 3, membrane deposition of complement and antibodies, and phagocytosis of parasitized erythrocytes. Br. J. Haematol. 113, 492–499 (2001)
Winterbourne, C. C. in CRC Handbook of Methods of Oxygen Radical Research (ed. Greenwald, R. A.) 137–141 (CRC Press, Boca Raton, 1985)
Acknowledgements
We thank our blood donors and J. F. Casella, B. Link, G. Rodgers, M. Law, K. D. Luc, N. Murray, J. A. Dvorak, F. Tokumasu, T. Arie, E. Fischer, L. H. Miller, A. Sadou, A. Katilé, B. Dakouo, K. Traoré and S. A. S. Diakité for their efforts in support of this work. H. F. acknowledges support from the United States Agency for International Development and the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Reprints and permissions information is available at npg.nature.com/reprintsandpermissions. The authors declare no competing financial interests.
Supplementary information
Supplementary Table S1
Median fluorescence intensities of parasitized erythrocyte populations probed with rat antisera. (DOC 78 kb)
Supplementary Table S2
Data demonstrating synchrony of the GB4 and 7G8 parasite lines in simultaneously infected AA and CC erythrocytes. (DOC 47 kb)
Rights and permissions
About this article
Cite this article
Fairhurst, R., Baruch, D., Brittain, N. et al. Abnormal display of PfEMP-1 on erythrocytes carrying haemoglobin C may protect against malaria. Nature 435, 1117–1121 (2005). https://doi.org/10.1038/nature03631
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1038/nature03631
This article is cited by
-
Effect of iron fortification on anaemia and risk of malaria among Ghanaian pre-school children with haemoglobinopathies and different ABO blood groups
BMC Nutrition (2023)
-
Single-molecule imaging and quantification of the immune-variant adhesin VAR2CSA on knobs of Plasmodium falciparum-infected erythrocytes
Communications Biology (2019)
-
Hemoglobin S and C affect biomechanical membrane properties of P. falciparum-infected erythrocytes
Communications Biology (2019)
-
Hemoglobin variants shape the distribution of malaria parasites in human populations and their transmission potential
Scientific Reports (2017)
-
Heterozygous HbAC but not HbAS is associated with higher newborn birthweight among women with pregnancy-associated malaria
Scientific Reports (2017)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
