
Abstract
Affect and craving are dynamic processes that are clinically relevant in opioid use disorder (OUD) treatment, and can be quantified in terms of intra-individual variability and stability. The purpose of the present analysis was to explore associations between opioid use and variability and stability of affect and craving among individuals receiving medication treatment for OUD (MOUD). Adults (N = 224) with OUD in outpatient methadone or buprenorphine treatment completed ecological momentary assessment (EMA) prompts assessing positive affect, negative affect, opioid craving, and opioid use. Dynamic structural equation modeling (DSEM) was used to quantify person-level indices of magnitude and stability of change. Beta regression was used to examine associations between intra-individual variability and stability and proportion of opioid-use days, when controlling for overall intensity of affect and craving. Results suggested that greater magnitude of craving variability was associated with opioid use on a greater proportion of days, particularly among individuals with lower average craving. Low average positive affect was also associated with higher proportion of days of use. Individuals who experience substantial craving variability in the context of lower average craving may be particularly vulnerable to opioid use during treatment. Ongoing assessment of craving may be useful in identifying treatment needs. Examining correlates of intra-individual variability and stability in MOUD treatment remains a relevant direction for future work.
Similar content being viewed by others

Introduction
Opioid use disorder (OUD) is associated with a tendency toward affective/cognitive states that, considered in a static fashion, would be summarized as low positive affect (PA), high negative affect (NA), and high craving for opioids. Each of these states is dynamic, and each might be better considered in terms of its stability (or variability) within each person. Specific patterns of intra-individual stability or variability have been observed in the context of internalizing and externalizing disorders [1], sleep [2], and chronic pain [3]. Specifically, internalizing disorders may be characterized by higher NA variability and lower PA variability, whereas externalizing disorders are associated with greater PA variability and instability [1]. Further, greater sleep variability often occurs in the context of depressive symptoms and stress [2]. Such patterns can manifest in ways that include (but are not limited to): (1) the amplitude or magnitude of change (i.e., the intra-individual standard deviation/iSD), and (2) temporal stability of specific states, or the extent to which an individual’s current state can be predicted by their previous one (i.e., autocorrelation/AR1).
An appreciation of such affective patterns in substance use might provide insights into outcomes that would be insufficiently understood if only evaluated in aggregate. Initial studies of affect and alcohol use dynamics have found that affective fluctuations are highest on days in which alcohol is consumed [4, 5], and fluctuations in affect and stress [6] are stabilized following alcohol use. Similarly, adolescents who showed greater mood variability at baseline increased their smoking over the course of a year, and increases in smoking were associated with stabilization in mood variability [7]. With some exceptions [8, 9], much of the work on affective variability and substance use has focused primarily on smoking or heavy drinking. Thus, extending this work to other populations, such as treatment-seeking populations and people with other addictive disorders (e.g., OUD), may provide further insight into risk and protective factors for substance use.
Additionally, other time-varying states, such as craving, remain largely unexplored using indices of stability and magnitude of variability. Craving is a diagnostic criterion for OUD in the DSM-5 [10], and negatively impacts treatment outcomes [11]. Previous work suggests that craving increases in the hours preceding opioid use [12,13,14]. These relationships are particularly strong in the presence of drug cues [15], stress [12,13,14], negative mood [14, 16], and pain [17]. However, individual differences in the magnitude and stability of craving fluctuation may also be clinically relevant. Indeed, within-person drug craving variability measured during 12 days of residential treatment for OUD has been linked with decreased odds of post-treatment substance use [9]. It may also be useful to examine craving variability and stability in the context of methadone or buprenorphine treatment (medication for OUD, MOUD). Although methadone and buprenorphine are gold-standard treatments for OUD and substantially attenuate craving, they do not completely eliminate craving [18]. Thus, we assessed the associations between dynamic craving variability patterns and opioid use in the context of MOUD treatments.
The aims of the present study were to explore whether intra-individual variability in affect and craving were associated with proportion of opioid use days during MOUD treatment. Using ecological momentary assessment (EMA), we examined intra-individual variability across two distinct but conceptually-relevant domains; the log(iSD2) (i.e., intra-indivdual magnitude of affective and craving variability) and the AR1 (i.e., intra-individual temporal stability across adjacent timepoints). It was expected that using opioids on a greater proportion of days would be associated with three indices of intra-individual variability: 1) greater magnitude of fluctuations in affect and craving, 2) greater instability in affect, and 3) greater persistence of craving. Exploratory analyses were conducted to examine interactions between these indices and average levels of affect and craving.
Materials and methods
Participants
Participants (N = 224) were recruited as part of a larger study of outpatients receiving methadone or buprenorphine treatment (administered daily) at the National Institute of Drug Abuse (NIDA) research clinic between July 2009 and June 2017. Participants attended the clinic 5–7 days per week and were provided supervised urine collection for drug screens 3 times per week. Eligibility criteria included 1) physical dependence on opioids, 2) age between 18–75, 3) no past or current psychotic disorder or bipolar disorder, 4) no current dependence on sedatives or alcohol, 5) no cognitive impairment or a medical condition that could interfere with study participation. The NIDA IRB approved the study.
Procedure
Participants were provided with a password-protected smartphone and were asked to complete 1) three random prompts per day that occurred during the patient’s waking hours, 2) event-contingent entries (e.g., drug-use events), and 3) end-of-day prompts. Participants were asked to respond within 15 min to random prompts. To maximize EMA compliance, participants were incentivized weekly for 1) provide EMA self-reports that matched urine drug-screen results given at the clinic ($3–10, depending on the parent study and whether the matched screen was positive or negative), which resulted in a strong correlation between UDS results and self-reported opoid use (r = 0.78, p < 0.001), and 2) completing at least 82% of random prompts (i.e., 23 out of 28 prompts per week). Participants also received a bonus for returning the smartphone at the end of the study. Participants who missed a substantial number of prompts were discharged from the study. Participants were assured that EMA reports would be seen only by investigators, not by clinic treatment staff.
The length of data collection spanned up to 30 weeks. However, we restricted analyses to the first 6 weeks of data collection in order to minimize the likelihood that intra-individual variability measures could be confounded by the length of time in treatment or number of assessments. The majority of participants had complete data during the first 6 weeks of data collection (M days in the study for first 6 weeks = 40.51, SD = 4.87). Participants were eligible for the present analysis if they had at least 2 weeks of EMA data.
Measures
Demographics
Participants reported their sex, age, race, and education level. The type of medication that the patient was receiving (methadone vs. buprenorphine) was extracted from electronic medical records.
Positive and negative affect
Participants rated their mood on a list of adjectives on a scale from 1 (Not at all) to 5 (Extremely) during random prompts. In line with previous factor analyses [14], the positive-affect items included carefree, happy, lively, cheerful, relaxed, contented, and pleased, and the negative-affect items included fatigued, worn out, afraid, annoyed, angry, hopeless, on edge, sad, discouraged, resentful, exhausted, and uneasy [14]. Responses were averaged to calculate a positive-affect and negative-affect score for each random-prompt entry.
Opioid craving
Participants indicated the extent to which they were craving heroin or other opioids within the past 5 min during random prompts on a scale from 1 (Not at all) to 5 (Extremely).
Opioid use
Participants were asked whether they had used heroin, other opioids, or street methadone or buprenorphine (in addition to treatment with MOUD) through three types of entries: 1) random prompts in which participants indicated whether they had used within 5 min of arriving at their location, 2) event-contingent entries in which participants logged drug-use events in near real-time, and 3) end-of-day prompts in which participants indicated whether there was any previously unrecorded use of heroin, opioid, or street methadone/buprenorphine that had occurred on that day. The outcome of this study is the proportion of days using opioids across the 6 weeks sampled.
Data analysis
For each variable (craving, NA, and PA), we first computed day-averages for each person, then person averages across days. We then calculated two person-level indices: intra-individual variances (iSD2) and autocorrelation (AR1). The iSD2 is an index of the magnitude of fluctuations of affective or craving states overall, whereas the AR1 is an index of temporal stability across successive timepoints (i.e., higher values reflect greater persistence of states, whereas lower values reflect greater transience [3]).
The iSD2 and AR1 were estimated by fitting a multilevel model using dynamic structural equation modeling (DSEM) framework in Mplus Version 8.6 [19]. DSEM presents a number of advantages over traditional multi-level models, including that the iSD and AR1 are estimated from latent variables and are thus free from measurement error. DSEM also uses latent variable centering, which can reduce likelihood of underestimating model parameters. Further, DSEM uses the discretization approach to make the time interval between observations approximately equal, and allows for level-1 residual variance to vary across individuals [3]. Note that Mplus provides log-transformed intra-individual variances [log(iSD2)] in order to meet the multivariate normal distribution assumption [3]. which we used for the rest of our analyses. Thus, the variability measures reported in the present study reflect log-transformed squared standard deviations across day-level measurements. Systematic cycles (e.g., weekends) may lead to violations of the assumption of stationarity (i.e., that the mean, variance, and autocorrelation are constant across timepoints). Thus, it is important to remove the influence of systematic trends prior to calculating intra-individual variability indices [3, 20]. To detrend the data, we adjusted for the linear effect of time by including day as an intra-subject predictor in the models. Based upon the suggestion by Hamaker et al. in conducting DSEM, we used a Bayesian estimator with 50,000 Markov Chain Monte Carlo iterations [21]. A total of six separate DSEM models were fit to estimate log(iSD2) and AR-1 for craving, NA, and PA. These values were then exported, and examined in relationship to our outcome variable (proportion of days on which the individual reported using any opioids during the first 6 weeks of data collection).
To contextualize the sample, bivariate correlations and t-tests were used as appropriate to examine bivariate relationships between demographic characteristics and study predictors (i.e., intra-individual variability measures and means). Next, bivariate correlations were conducted to explore relationships between study predictors. To test the main hypotheses that indices of intra-individual variability in affect and craving (predictors) would be associated with proportion of opioid use days during 6 weeks of treatment (outcome), we conducted a series of extended beta regression analyses. Beta regression is a form of regression analysis intended for proportional outcome data that bound from 0 to 1; it can also account for heteroskedasticity and skewness without transformation of the outcome data [22]. Extended beta regression is a special case of beta regression that provides better parameter estimates by not assuming that the precision parameter (i.e., inverse measure of dispersion of the outcome) is constant [23,24,25]. Extended beta regression provides two sub-models: 1) a mean sub-model, and 2) a precision sub-model. The mean sub-model provides information about the effects of predictors on the outcome’s mean, whereas the precision sub-model provides information about the effects of predictors on the outcome’s dispersion [24, 25]. The betareg package in R was used for all extended beta regression analyses [26].
Beta regression models were fit systematically. First, for each beta-regression analysis, two variables were entered as predictors: 1) the log(iSD2) value or the AR1 value, and 2) the mean value (e.g., person-average PA, NA, or craving). This process was then repeated for each set of predictor variables. We present both unadjusted models, and models adjusting for relevant demographic (sex and age) and clinically relevant (medication type: methadone or buprenorphine) characteristics. Next, we tested for an interaction between average values and intra-individual variability measures. If the interaction was statistically significant, we conducted the Johnson–Neyman approach as a follow-up test. Finally, we fit a final beta-regression model that included variability measures significantly related to the outcome. This final analysis also controlled for averages, as well as relevant demographic and treatment characteristics. Due to the multiple comparisons used in the present study, the Benjamini–Hochberg procedure was used to adjust for the false discovery rate [27].
Results
EMA adherence/completion rates
During the 6-week time period explored in the present analysis, participants responded to 22,304 out of 27,228 random prompts possible (81.9% completion rate), an average of 99.57 per person (SD = 21.88), resulting in an average of 37.80 (SD = 6.29) days of random-prompt data per person. Opioid-use reports were available for an average of 38.45 days per person (SD = 5.92).
Descriptive information and bivariate relationships between study predictors
Descriptive information about the sample is presented in Table 1. Bivariate relationships between study predictors are shown in Table 2. Correlations between person-mean and intra-individual variability measures for the same scale ranged from small to large. In addition to the relationships described in the table, it should be noted that age was significantly positively related to average PA (r = 0.18, p = 0.008), but was not significantly related to other study predictors (rs < 0.14, ps > 0.043). Intensity, variability, and stability of PA, NA, and craving did not vary by sex (ps > 0.126) or type of medication treatment (methadone vs. buprenorphine) (ps > 0.267).
Affect and craving variability and stability and opioid use days
Results from beta regression analyses are presented in Table 3. Individuals who experienced a greater magnitude of fluctuations in craving and individuals with lower average PA reported using opioids on a greater proportion of days. These relationships remained significant when controlling for demographic and clinically relevant covariates. Age (Bs = 0.03, all ps < 0.001) and OUD medication (buprenorphine vs. methadone treatment; Bs > 0.46, ps < 0.009) were also associated with proportion of days of use.
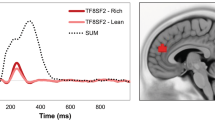
When interaction terms were added to the model, there was a significant interaction between average craving and the log(iSD2) of craving (B = −0.46, p < 0.001). Follow-up tests using the Johnson-Neyman formula suggested that the slope of the Craving log(iSD2) was significant (p < 0.01) and positive at levels of average craving below 1.18 (65th percentile), as shown in Fig. 1 (i.e., increased craving variability was associated with greater opioid use only at very low levels of craving). In contrast, the Craving log(iSD2) was also significant and negative at average levels of craving above 3.30 (99th percentile), though it should be noted that very few participants (N = 2) fell within this range, and this finding should be interpreted with caution given the small number of data points. As a sensitivity analysis, we re-ran this analysis using a winsorized average craving variable due to positive skew in the average craving variable. Results were virtually unchanged. Interaction term = B = −0.47, p = 0.002, Johnson–Neyman interval = 1.17–4.45.) The interaction of average craving and the AR1 of craving approached, but did not reach, significance (B = −0.79, p = 0.074).

Johnson–Neyman plot depicting the slope of craving variability and proportion of opioid use days (slope plotted on vertical axis) as a function of mean levels of craving (horizontal axis). The slope of craving log(iSD2) was only significant (p < 0.01) and positive at levels of average craving below 1.18 (65th percentile). The slope of craving log(iSD2) was also significant and negative at average levels of craving that were high relative to the rest of the sample (above the 99th percentile, data not shown in this figure).
Final extended beta regression model
In the final model, presented in Table 4, we entered variables found to be significantly associated with proportion of days of opioid use in earlier models (i.e., average PA, average craving, and craving log(iSD2)) into the same extended beta regression model, while controlling for sex, age, and medication type. Craving log(iSD2) and lower average PA remained positively associated with proportion of opioid-use days, whereas average craving did not. The interaction of craving log(iSD2) and average craving also remained significant when added to the model, with follow-up tests suggesting a similar pattern in which the slope of the craving log(iSD2) was related to proportion of days of opioid use at the p < 0.01 level at average levels of craving below 1.16 (63.8th percentile).
Discussion
The purpose of the present analysis was to examine relationships between opioid use and two dimensions of intra-individual affect and craving variability (magnitude of change and temporal stability) among outpatients in MOUD treatment. Results indicated that greater magnitude of craving variability was significantly associated with opioid use, particularly among individuals with lower average craving. In contrast, measures of affective variability were largely unrelated to use, although higher average positive affect was associated with lower opioid use. Negative affect was not associated with opioid use. Further, stability of affect and craving was not related to opioid use.
Published studies have reported an inconsistent relationship between craving and substance use [28]. However, studies using EMA have been more consistent in detecting the clinical significance of craving and use across a number of substances [12,13,14, 29]. This paper approached craving assessment from a different analytical perspective; examining individual differences in magnitude of craving variability and stability of craving, while controlling for average intensity of craving. There are some tradeoffs to examining craving and opioid use through indices of variability and stability, instead of through a more traditional means-based approach with mixed-effects models. For example, variability/stability methods using dynamic structural equation modeling describe patterns of association over time, whereas means-based mixed-effects models can provide more granular information about momentary associations between craving and opioid use. Nonetheless, there are some notable benefits to calculating indices of variability and stability. For example, the methodology employed in the present study allows for quantification of individual differences in the course of symptoms during treatment. Results from the present study suggest that even among individuals in treatment for OUD whose craving is attenuated by medication, there is substantial variation across individual patterns of variability and stability. These different patterns, and relationships with treatment outcomes, underscore the extent to which individuals with distinct symptom profiles may have different clinical needs and use patterns.
Although a substantial number of participants experienced low or no craving on a majority of days, some participants experienced days with high craving. Participants who fit that pattern (i.e., generally low craving, but high magnitude of craving variability) were more likely to use opioids on a larger proportion of days than those who had higher but less variable craving. The opposite pattern was observed among individuals with higher average craving (in which greater craving variability was associated with lower likelihood of use). However, this finding should be interpreted with caution due to the small number of individuals who experienced low opioid use in the context of high intensity and variability of craving. This question may be explored in future research by specifically recruiting individuals who identify high craving as a treatment target, and exploring relationships between variability and use among this population. Craving stability (i.e., the AR1) was not related to proportion of opioid use days. It may be that persistence of craving (i.e., difficulty returning to baseline) as well as craving instability (i.e., unexpected changes in craving) may each be related to opioid use among different individuals, and may represent distinct subtypes of individuals at risk for use.
Craving can be elicited by stress [13, 15, 30], drug cues [15], and pain [17], as we and others have shown via EMA. Future work should extend these findings by understanding 1) the mechanisms that cause some people to have larger magnitudes of variability in craving, 2) clinical correlates (e.g., co-occurring psychiatric comorbidity) of larger craving variability and stability, and 3) directionality between relationships. Bivariate analyses in the present study showed that craving variability was related to higher average negative affect, lower average positive affect, and greater magnitude of negative-affect variability. These findings suggest that individuals who experience greater magnitude of craving variability may also be prone to 1) general affective distress, and 2) experiencing difficulties with emotion regulation, phenotypes that are characteristic of patients with OUD [31]. Indeed, craving may be manifested as anticipation of negative reinforcement from a substance [32], itself a dynamic process. Future studies are warranted to explore the hypothesis that magnitude of craving variability is related to greater psychiatric comorbidity and difficulties with regulating emotions, or that craving variability mediates the relationship between affect instability and opioid use.
Low average PA was also related to higher proportion of days of use in the present study, consistent with previous work [33]. This finding is in line with principles of psychological treatments which encourage increasing positive affect through identification of alternate reinforcers, including cognitive behavior therapy [34], dialectical behavior therapy [35], and the Community Reinforcement Approach [36]. In contrast, affective-variability measures (both positive and negative) were not related to opioid use. These findings are somewhat consistent with prior findings that daily positive and negative moods, modeled separately, were not associated with greater odds of alcohol use [4]. Further, NA was not related to opioid use. Recent work suggests that certain diagnoses characterized by high negative affect, such as depressive symptoms, are inconsistently related to OUD treatment outcomes [37, 38], a phenomenon that should be explored further. Of note, the present study collapsed across a range of PA and NA states, using a factor-analytic strategy we have described elsewhere [14]. Because specific emotions within the broader umbrella of PA or NA may differ in arousal or transience, and because specific domains of NA (i.e., depression) have been inconsistently related to use [37, 39], future work should explore dynamics of specific emotional states (e.g., sadness vs. anger).
Findings from the present analysis also have implications for clinical practice. Because craving is a diagnostic criterion for OUD [10] and a target of gold-standard OUD medications [40], clinicians may be most concerned about patients who report persistent high cravings. However, findings from the present study suggest that spikes in craving can occur even among patients whose typical levels of craving are low. For these patients, continued assessment of craving, relapse prevention planning [41], and distress-tolerance skills [35] may be beneficial for management of craving when it arises. For instance, it may be useful to ask patients about “maximum craving” in addition to “typical craving.” Of note, however, because of the correlational nature of our analyses, we cannot ascertain that reducing spikes of craving will necessarily reduce use. Indeed, this possibility should be balanced with the notion that cessation of use will stabilize craving. Nonetheless, craving is an aversive state for many patients, and reducing unexpected increases in craving may improve patient well-being. Further, future research may test the potential utility of integrating EMA into clinical practice. For example, clinicians could potentially collect data through EMA to provide patients feedback about their craving patterns, as well as to inform interventions for use.
Limitations
This study should be interpreted in the context of certain limitations. Data were collected from participants in treatment at a single clinic and may not be generalizable to other geographic regions or clinic settings. Study candidates with serious mental illness (i.e., bipolar disorder or a psychotic disorder) and those physically dependent on alcohol or sedatives were excluded, and results may not generalize to these populations. Because methadone and buprenorphine attenuate craving [40], results may not generalize to patients with OUD who are not in MOUD treatment. However, ongoing craving during MOUD is a clinically important issue. Additionally, there are a number of factors that may influence craving in the context of MOUD treatment that we were not able to account for in this study, including if a patient missed a dose or metabolized methadone or buprenorphine rapidly. These factors, as well as whether different symptom patterns are observed in different types of medication treatment, should be explored in future work. Future studies should also follow up with participants to see if the findings of the present study align with participants’ perceptions of use patterns (i.e., that spikes in craving preceded use).
Further, it should be noted that our findings are fundamentally cross-sectional because intra-individual variability indices are calculated at the person level, and thus, we cannot determine directionality of relationships. Findings from the alcohol use literature suggest that mood instability may increase before drinking events and stabilize after drinking events [42]. It may be beneficial to collect a greater number of within-day assessments in order to capture whether craving instability increases in the hours leading up to opioid-use events or in response to drug cues or stressful events. There are tradeoffs to this approach, such as potential response habituation and the necessity to reduce the overall number of days assessed. Finally, future studies that aim to collect measures of intra-individual variability, particularly those that are recruiting participants within a single geographic region in the same time frame, should consider testing the extent to which cultural stressors (e.g., presidential elections) influence variability indices.
Conclusions
This analysis examined intra-individual variability indices for both affect and craving in outpatients being treated with MOUD. Results suggest that patients with greater variability in craving, especially if their average craving is low, are more likely to use opioids on a greater proportion of days than those with less variable craving. Future research should aim to help determine directionality of these relationships; it is possible that helping patients modulate craving on days when craving deviates from their average may be beneficial in clinical practice. It is also possible that helping patients stop using opioids may reduce unexpected spikes in craving, an aversive experience for patients. Future studies should also 1) identify correlates of high craving variability, and 2) examine whether findings replicate for other substances, and for patients with OUD who are not taking medications.
Change history
05 July 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41386-022-01372-8
References
Scott L, Victor S, Kaufman E, Beeney J, Byrd A, Vine V, et al. Affective dynamics across internalizing and externalizing dimensions of psychopathology. Clin Psychol Sci. 2020;8:412–27.
Bei B, Wiley J, Trinder J, Manber R. Beyond the mean: a systematic review on the correlates of daily intraindividual variability of sleep/wake patterns. Sleep Med Rev. 2016;28:108–24.
Mun C, Suk H, Davis M, Karoly P, Finan P, Tennen H, et al. Investigating intraindividual pain variability: methods, applications, issues, and directions. Pain. 2019;160:2415–29.
Gottfredson N, Hussong A. Drinking to dampen affect variability: findings from a college student sample. J Stud Alcohol Drugs. 2013;74:576–83.
Jahng S, Solhan M, Tomko R, Wood P, Piasecki T, Trull T. Affect and alcohol use: an ecological momentary assessment study of outpatients with borderline personality disorder. J Abnorm Psychol. 2011;120:572–84.
Dvorak R, Stevenson B, Kilwein T, Sargent E, Dunn M, Leary A, et al. Tension reduction and affect regulation: an examination of mood indices on drinking and non-drinking days among university student drinkers. Exp Clin Psychopharmacol. 2018;26:377–90.
Weinstein S, Mermelstein R, Shiffman S. Mood variability and cigarette smoking escalation among adolescents. Psychol Addict Behav. 2008;22:504–13.
McKee K, Russell M, Mennis J, Mason M, Neale M. Emotion regulation dynamics predict substance use in high-risk adolescents. Addict Behav. 2020;106:106374.
Cleveland H, Knapp K, Brick T, Russell M, Gajos J, Bunce S. Effectiveness and utility of mobile device assessment of subjective craving during residential opioid dependence treatment. Subst Use Misuse. 2021;56:1284–94.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. United States: American Psychiatric Association.; 2013.
Tsui J, Anderson B, Strong D, Stein M. Craving predicts opioid use in opioid-dependent patients initiating buprenorphine treatment: a longitudinal study. Am J Drug Alcohol Abus. 2014;40:163–9.
Burgess-Hull A, Smith K, Schriefer D, Palilio L, Epstein D, Preston K. Longitudinal patterns of momentary stress during outpatient opioid agonist treatment: A growth-mixture-model approach to classifying patients. Drug Alcohol Depend. 2021;226:108884.
Panlilio L, Stull S, Bertz J, Burgess-Hull A, Lanza S, Curtis B, et al. Beyond abstinence and relapse II: momentary relationships between stress, craving, and lapse within clusters of patients with similar patterns of drug use. Psychopharmacology. 2021;238:1513–29.
Preston K, Kowalczyk W, Phillips K, Jobes M, Vahabzadeh M, Lin L, et al. Before and after: craving, mood, and background stress in the hours surrounding drug use and stressful events in patients with opioid-use disorder. Psychopharmacology. 2018;235:2713–23.
Preston K, Kowalczyk W, Phillips K, Jobes M, Vahabzadeh M, Lin J, et al. Exacerbated craving in the presence of stress and drug cues in drug-dependent patients. Neuropsychopharmacology. 2018;43:859–67.
Kowalczyk W, Moran L, Bertz J, Phillips K, Ghitza U, Vahabzadeh M, et al. Using ecological momentary assessment to examine the relationship between craving and affect with opioid use in a clinical trial of clonidine as an adjunct medication to buprenorphine treatment. Am J Drug Alcohol Abus. 2018;44:502–11.
Mun C, Finan P, Epstein D, Kowalczyk W, Agage D, Letzen J, et al. Craving mediates the association between momentary pain and illicit opioid use during treatment for opioid-use disorder: An ecological momentary assessment study. Addiction. 2021;116:1794–804.
Kakko J, Alho H, Baldacchino A, Molina R, Nava F, Shaya G. Craving in opioid use disorder: from neurobiology to clinical practice. Front Psychiatry. 2019;10:592.
Muthén LK, Muthén BO. Mplus user’s guide. Eighth Edition. Los Angeles, CA: Muthén & Muthén (1998–2017).
Wang L, Hamaker E, Bergeman C. Investigating inter-individual differences in short-term intra-individual variability. Psychol Methods. 2012;17:567–81.
Hamaker E, Asparouhov T, Brose A, Schmiedek F, Muthén B. At the frontiers of modeling intensive longitudinal data: dynamic structural equation models for the affective measurements from the COGITO study. Multivar Behav Res. 2018;3171:1–22.
Cribari-Neto F, Zeileis A. Beta regression in R. J Stat Softw. 2010;32:1–24.
Bayer F, Cribari-Neto F. Model selection criteria in beta regression with varying dispersion. Commun Stat-Simul Comput. 2017;46:729–46.
Smithson M, Verkuilen J. A better lemon squeezer? Maximum-likelihood regression with beta-distributed dependent variables. Psychol Methods. 2006;11:54–71.
Hunger M, Baumert J, Holle R. Analysis of SF-6D index data: is beta regression appropriate? Value Health. 2011;14:759–67.
Zeileis A, Caribari-Neto F, Gruen B, Kosmidis I, Simas A, Rocha A, et al. Package ‘betareg’. 2016.
Thissen D, Steinberg L, Kuang D. Quick and easy implementation of the Benjamini-Hochberg procedure for controlling the false positive rate in multiple comparisons. J Educ Behav Stat. 2002;27:77–83.
Tiffany S, Wray J. The clinical significance of drug craving. Ann NY Acad Sci. 2012;1248:1–17.
Serre F, Fatseas M, Swendsen J, Auriacombe M. Ecological momentary assessment in the investigation of craving and substance use in daily life: a systematic review. Drug Alcohol Depend. 2015;148:1–20.
Preston K, Epstein D. Stress in the daily lives of cocaine and heroin users: relationship to mood, craving, relapse triggers, and cocaine use. Psychopharmacology. 2011;218:29–37.
Garland E, Bryan C, Nakamura Y, Foreliger B, Howard M. Deficits in autonomic indices of emotion regulation and reward processing associated with prescription opioid use and misuse. Psychopharmacology. 2017;234:621–9.
Bergeria C, Strickland J, Huhn A, Strain E, Dunn K. A preliminary examination of the multiple dimensions of opioid craving. Drug Alcohol Depend. 2021;219:108473.
Kiluk B, Yip S, DeVito E, Carroll K, Sofuoglu M. Anhedonia as a key clinical feature in the maintenance and treatment of opioid use disorder. Clin Psychol Sci. 2019;7:1190–206.
McHugh R, Hearon B, Otto M. Cognitive-behavioral therapy for substance use disorders. Psychiatr Clin. 2010;33:511–25.
Linehan M. DBT skills training manual. Guilford Publications; 2014.
Miller WR, Meyers RJ, Hiller-Sturmhöfel S. The community-reinforcement approach. Alcohol Research & Health. 1999;23:116–21.
Ghabrash M, Bahremand A, Veileuz M, Blais-Normandin G, Chicoine G, Sutra-Cole C, et al. Depression and outcomes of methadone and buprenorphine treatment among people with opioid use disorders: a literature review. J Dual Diagn. 2020;16:191–207.
Ellis J, Rabinowitz J, Wells J, Liu F, Finan P, Stein M, et al. Latent trajectories of anxiety and depressive symptoms among adults in early treatment for nonmedical opioid use. J Affect Disord. 2022;299:223–32.
Zhu Y, Mooney L, Yoo C, Evans E, Kelleghan A, Saxon A, et al. Psychiatric comorbidity and treatment outcomes in patients with opioid use disorder: results from a multisite trial of buprenorphine-naloxone and methadone. Drug Alcohol Depend. 2021;228:108996.
Petitjean S, Stohler R, Déglon J, Livoti S, Waldvogel D, Uehlinger C, et al. Double-blind randomized trial of buprenorphine and methadone in opiate dependence. Drug Alcohol Depend. 2001;62:97–104.
Marlatt G, George W. Relapse prevention: introduction and overview of the model. Br J Addict. 1984;79:261–73.
De Leon A, Dvorak R, Kramer M, Peterson R, Pinto D, Leary A, et al. Daily patterns of emotional functioning on drinking and nondrinking days. Alcohol Clin Exp Res. 2020;44:2598–610.
Funding
This study was supported by the Intramural Research Program of the National Institute on Drug Abuse, National Institutes of Health and the National Institute on Drug Abuse T32 DA007209 (Strain, Bigelow, Weerts) and F32 DA04939302 (Mun).
Author information
Authors and Affiliations
Contributions
JDE: Conceptualization, formal analysis, visualization, writing—original draft.; CJM: Conceptualization, formal analysis, visualization, writing—original draft; DHE: Methodology, data curation, writing—review & editing, project administration; KAP: Writing—review & editing, project administration; PAF: Conceptualization, supervision, writing—review & editing; KLP: Investigation, resources, writing—review & editing, project administration, funding acquisition.
Corresponding authors
Ethics declarations
Competing interests
PHF is on the scientific advisory board for Ninnion. The other authors report no conflicts of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised to correct typos in the abstract and results section.
Rights and permissions
About this article

Cite this article
Ellis, J.D., Mun, C.J., Epstein, D.H. et al. Intra-individual variability and stability of affect and craving among individuals receiving medication treatment for opioid use disorder. Neuropsychopharmacol. 47, 1836–1843 (2022). https://doi.org/10.1038/s41386-022-01352-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41386-022-01352-y
This article is cited by
-
A mixed methods experience sampling study of a posttraumatic growth model for addiction recovery
Scientific Reports (2024)
-
Examining Associations Between Negative Affect and Substance Use in Treatment-Seeking Samples: a Review of Studies Using Intensive Longitudinal Methods
Current Addiction Reports (2022)
