
Abstract
TNNI3 is a gene that causes hypertrophic cardiomyopathy (HCM). A 14-year-old girl who was diagnosed with nonobstructive HCM presented with cardiopulmonary arrest due to ventricular fibrillation. Genetic testing revealed a novel de novo heterozygous missense variant in TNNI3, NM_000363.5:c.583A>T (p.Ile195Phe), which was determined to be the pathogenic variant. The patient exhibited progressive myocardial fibrosis, left ventricular remodeling, and life-threatening arrhythmias. Genetic testing within families is useful for risk stratification in pediatric HCM patients.
Similar content being viewed by others


Hypertrophic cardiomyopathy (HCM) is characterized by left ventricular (LV) hypertrophy and diastolic dysfunction, and it is the most common inherited cardiovascular disease. Approximately half of patients with genetically identified HCM have a family history of the disease, which follows an autosomal dominant mode of inheritance. Many disease-causing pathological variants have been identified in genes encoding sarcomere proteins, which are the contractile units of the myocardium. The prevalence of HCM is estimated to be at least 1 in 500 in the general population1,2, and advancements in diagnostic methods such as imaging and genetic analysis have increased its diagnosis. Recent research suggests that 1 in 200 people may have HCM3.
Nonobstructive HCM is common among patients with HCM and is typically well tolerated. However, a small number of patients may experience disease progression, which is characterized by LV remodeling, leading to thinning of the LV wall with diffuse replacement scarring; in some cases, sudden cardiac death may occur as the initial manifestation4,5,6. A previous study showed that patients diagnosed with HCM at a young age have a worse prognosis than those diagnosed as adults, with sudden death occurring approximately twice as often2. Therefore, early diagnosis and prediction of the severity of pediatric cardiomyopathy are crucial2,7. In this report, we present the case of a patient with a novel TNNI3 heterozygous variant who was diagnosed with nonobstructive HCM and experienced progressive myocardial fibrosis, LV structural remodeling, and life-threatening arrhythmias during the follow-up period.
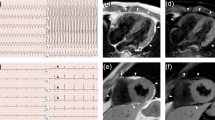
The patient was a 14-year-old girl who was asymptomatic and lacked any family history of cardiomyopathy, including sudden death or cardiac hypertrophy (Fig. 1A). Abnormal electrocardiographic findings were incidentally discovered during a routine school physical examination, and subsequent evaluation with echocardiogram and cardiac magnetic resonance imaging (MRI) confirmed the diagnosis of HCM. Echocardiography at the time of diagnosis revealed preserved LV contractility, with an LV ejection fraction of 65% and no evidence of abnormal wall motion, and heterogeneous wall thickening was observed primarily in the inferoseptal area, with a maximum wall thickness of 15 mm. Cardiac MRI examination did not show any evidence of myocardial edema or late gadolinium enhancement (LGE) (Fig. 1B, a–c). A treadmill exercise test conducted for risk assessment did not reveal any ventricular arrhythmias, and dobutamine stress echocardiography did not show any findings suggestive of an obstructed outflow tract. Consequently, she underwent regular follow-up without aggressive treatment, including drug therapy. Approximately one year into the follow-up period, she suffered cardiac arrest due to ventricular fibrillation while running up the stairs at school and was successfully resuscitated. Following transportation to the hospital, cardiac MRI revealed no change in the degree of wall thickening; however, new myocardial edema was detected in the thickened inferoseptal area and the anterolateral wall (Fig. 1B, d, e). Furthermore, LGE corresponded to the area of myocardial edema (Fig. 1B, f). During her hospital stay, she underwent subcutaneous implantable cardioverter-defibrillator (S-ICD) implantation, and beta-blockers were initiated. After 12 months, a stress test (involving cardiopulmonary and treadmill stress tests), echocardiogram, and cardiac MRI were performed, revealing no significant progression of her cardiac condition.

A Family pedigree showing the inheritance pattern of cardiomyopathy. Squares represent males, and circles represent females. The black symbols indicate affected individuals, and the open symbols indicate unaffected individuals. The arrow indicates the proband who was diagnosed with hypertrophic cardiomyopathy (HCM). P, proband; E, genetic evaluation; +, presence of TNNI3 variant; −, absence of TNNI3 variant. B Cardiac magnetic resonance images of short-axis cine (a, d), T2-weighted (b, e), and late gadolinium enhancement (LGE) (c, f) images at the time of HCM diagnosis (a–c) and after resuscitation (d–f). a, d Left ventricular wall thickness exhibited heterogeneity, with a maximum thickness of 15 mm. No change in the degree of wall thickening was observed. b, c There was no myocardial edema. (e and f) Areas with high T2 signals were observed in the inferoseptal area and anterolateral wall (e) and corresponded to those of LGE (arrow).
After resuscitation, whole-exome sequencing was performed after obtaining written consent from the patient and her parents. A heterozygous missense variant, c.583A>T (p.Ile195Phe), was detected in exon 8 of TNNI3 (NM_000363.5), which encodes troponin I, a cardiac sarcomere component and subtype of troponin. This variant was not previously reported in the Genome Aggregation Database (gnomAD: URL: http://gnomad.broadinstitute.org/) or in the Japanese genome databases jMorp3 and HGVD8. This variant was absent in her healthy parents, indicating a de novo occurrence (Fig. 2A). In silico analysis was used to predict the effects of the variant on protein function using a combination of Alpha Missense9 and dbNSFP10. The Alpha Missense score was 0.9259, suggesting a likely pathogenic nature. The CADD score was 23.3, the SIFT score was 0.001 (damaging), and the FATHMM score was 0.891 (damaging), all indicating potential pathogenicity. Approximately 80% of reported pathological variants of TNNI3 are located in exons 7 and 8, which encode the domains that interact with myocardial actin and cardiac troponin C, which are sarcomere components11. TNNI3 c.583A>T (p.Ile195Phe) was also located in exon 8 (Fig. 2B)12. Thus, the variant identified in this study can be classified as a likely pathogenic variant because it met the PS2, PM1, PM2, and PP3 criteria of the American College of Medical Genetics and Genomics/Association for Molecular Pathology (ACMG/AMP) guidelines13.

A Sanger sequencing results for the TNNI3 (NM_000363.5) gene in the parents (II-1, II-4) and the patient (III-1). The patient carries a heterozygous missense variant, c.583A>T, p.Ile195Phe. B TNNI3 pathogenic variants associated with HCM previously reported in ClinVar (URL: https://www.ncbi.nim.nih.gov/clinvar/) are shown in the form of a lollipop plot. The red plot represents the variant identified in this patient, located in exon 8.
The calcium sensitivity of myocardial contraction is regulated by the troponin complex, which comprises three subunits: troponin I, troponin C, and troponin T. TNNI3, which encodes cardiac troponin I, the inhibitory component of myocardial contractility, plays a key role in regulating myocardial contraction and relaxation in response to fluctuations in intracellular calcium levels4. The prevalence of pathological variants of TNNI3 is reportedly less than 5% in patients with cardiomyopathies, with a relatively low penetrance of approximately 50%5,6. However, its phenotype presents challenges for prognosis and risk assessment owing to the heterogeneity of the onset times and phenotypes even within the same family. Patients with pathological variants of TNNI3 reportedly experience severe clinical outcomes, such as fatal arrhythmias and sudden death, even in children7,14.
This case involved a patient with de novo pediatric HCM who experienced fatal arrhythmia during the follow-up period, necessitating the insertion of an ICD for secondary prevention after resuscitation. Accurately predicting disease severity solely based on clinical examination at the time of diagnosis remains challenging. Pediatric HCM, although less commonly diagnosed in clinical practice, is associated with a more severe disease status than adult HCM15.
HCM is one of the major causes of sudden cardiac death in childhood7,11, and individuals diagnosed with HCM during childhood have a poorer prognosis than those diagnosed in adulthood16. Moreover, 90% of pediatric HCM patients who undergo ICD insertion have been reported to have de novo variants6. De novo variants are a major cause of severe early-onset genetic diseases17. Genetic testing plays a crucial role in identifying clinically diagnostic genetic factors associated with HCM, particularly in young populations. However, genetic testing typically focuses only on proband analysis, and comprehensive family genetic evaluation is still underutilized in clinical practice, potentially leading to failure in identifying pathogenic variants. Thus, in de novo pediatric HCM patients, variants identified in disease-related genes through family genetic testing may have a significant influence on phenotypic development.
Although patients with HCM have multiple potential life-threatening factors that contribute to disease severity and sudden cardiac death, identifying high-risk patients, particularly children with HCM, remains challenging16. Therefore, genetic testing within families can be useful for risk stratification and treatment optimization, especially for preventing sudden cardiac death in pediatric HCM patients.
HGV Database
The relevant data from this Data Report are hosted at the Human Genome Variation Database at https://doi.org/10.6084/m9.figshare.hgv.3382.
References
Maron, B. J., Haas, T. S., Ahluwalia, A., Murphy, C. J. & Garberich, R. F. Demographics and epidemiology of sudden deaths in young competitive athletes: from the united states national registry. Am. J. Med 129, 1170–1177 (2016).
Lipshultz, S. E. et al. Risk stratification at diagnosis for children with hypertrophic cardiomyopathy: an analysis of data from the Pediatric Cardiomyopathy Registry. Lancet 382, 1889–1897 (2013).
Tadaka, S. et al. jMorp: Japanese Multi-Omics Reference Panel update report 2023. Nucleic Acids Res. 46, D551–D557 (2023).
Gomes, A. V. & Potter, J. D. Molecular and cellular aspects of troponin cardiomyopathies. Ann. N. Y Acad. Sci. 1015, 214–224 (2004).
Mogensen, J. et al. Frequency and clinical expression of cardiac troponin I mutations in 748 consecutive families with hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 44, 2315–2325 (2004).
van den Wijngaard, A. et al. Recurrent and founder mutations in the Netherlands: cardiac Troponin I (TNNI3) gene mutations as a cause of severe forms of hypertrophic and restrictive cardiomyopathy. Neth. Heart J. 19, 344–351 (2011).
Bagnall, R. D. et al. Genetic basis of childhood cardiomyopathy. Circ. Genom. Precis Med. 15, e003686 (2022).
Higasa, K. et al. Human genetic variation database, a reference database of genetic variations in the Japanese population. J. Hum. Genet. 61, 547–553 (2016).
Cheng, J. et al. Accurate proteome-wide missense variant effect prediction with AlphaMissense. Science 381, eadg7492 (2023).
Liu, X., Li, C., Mou, C., Dong, Y. & Tu, Y. dbNSFP v4: a comprehensive database of transcript-specific functional predictions and annotations for human nonsynonymous and splice-site SNVs. Genome Med. 12, 103 (2020).
Maron, B. J., Doerer, J. J., Haas, T. S., Tierney, D. M. & Mueller, F. O. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation 119, 1085–1092 (2009).
Jay, J. J. & Brouwer, C. Lollipops in the clinic: information dense mutation plots for precision medicine. PLoS ONE 11, e0160519 (2016).
Richards, S. et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med 17, 405–424 (2015).
Hong, Y., Su, W. W. & Li, X. Risk factors of sudden cardiac death in hypertrophic cardiomyopathy. Curr. Opin. Cardiol. 37, 15–21 (2022).
Hayashi, T. et al. Genetic background of Japanese patients with pediatric hypertrophic and restrictive cardiomyopathy. J. Hum. Genet. 63, 989–996 (2018).
Semsarian, C., Ingles, J., Maron, M. S. & Maron, B. J. New perspectives on the prevalence of hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 65, 1249–1254 (2015).
Acuna-Hidalgo, R., Veltman, J. A. & Hoischen, A. New insights into the generation and role of de novo mutations in health and disease. Genome Biol. 17, 241 (2016).
Acknowledgements
The authors extend their gratitude to Tomohiro Umezu for their technical assistance in conducting whole-exome and Sanger sequencing. This work was supported by the Japan Society for the Promotion of Science KAKENHI, grant number 21K08089 (N.I.).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Inagaki, N., Okano, T., Kobayashi, M. et al. Pediatric hypertrophic cardiomyopathy caused by a novel TNNI3 variant. Hum Genome Var 11, 14 (2024). https://doi.org/10.1038/s41439-024-00272-1
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41439-024-00272-1
